The Science
Waist circumference predicts lifespan. Muscle is the organ of longevity. Hunger is a mineral deficit, not a need for GLP-1s. The cutting-edge science that maximizes your longevity — and makes you unstoppable.

01 · Fasting, Belly Fat & Longevity
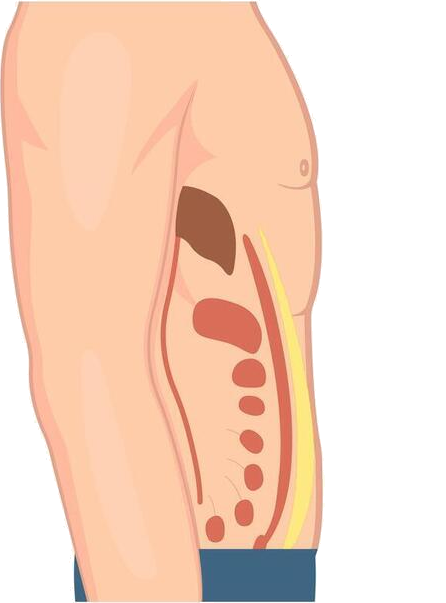
The fat around your middle is the fat that matters.
Visceral fat — the fat packed around your organs, hidden beneath the outer subcutaneous layer — is one of the strongest predictors of premature death, more telling than weight or BMI alone. The good news: it responds to when you eat, not just what.
An 8-hour eating window cuts visceral fat — as sustainably as cutting calories.
Time-restricted eating reduced visceral fat comparably to daily calorie restriction in a randomized trial. The fasting hours also trigger autophagy, the cell's natural cleanup.
Waist size tracks with how long you live.
In large cohorts, a larger waist circumference predicted higher all-cause mortality independent of BMI.
Sugar feeds visceral fat; salt does not.
Fructose-sweetened drinks increased visceral fat and worsened insulin sensitivity in a controlled trial — which is why the protocol is sugar-free by design. Remove the sugar, keep the salt.
Bonus · Watch
The day Dr. Oz measured my belly.
2008, Columbia University. The on-air moment Dr. Oz measured Jorge's waist — and made visceral belly fat impossible to ignore.
▶ Watch the moment →
Bonus · Read
Your waistline is your lifeline.
Why your waist — not the scale — is the number that tracks with how long you live.
Read it on Substack →
02 · Muscle, Sarcopenia & Longevity
Muscle is the organ of longevity.
A small waist is half the equation. The other half is lean muscle — and there are two kinds. Skeletal muscle is the muscle you can see and train in the gym: the glucose sink, the frame that keeps you upright and independent. Cardiovascular muscle is the heart and the vast capillary network that feeds every working fiber with oxygen — measured as VO₂ max. After 40, adults lose roughly 3–8% of skeletal muscle per decade if they do nothing, and cardiorespiratory fitness declines in parallel. Both losses predict frailty, falls, and early decline. Both can be reversed at almost any age.
74 · No resistance training
74 · Resistance-trained
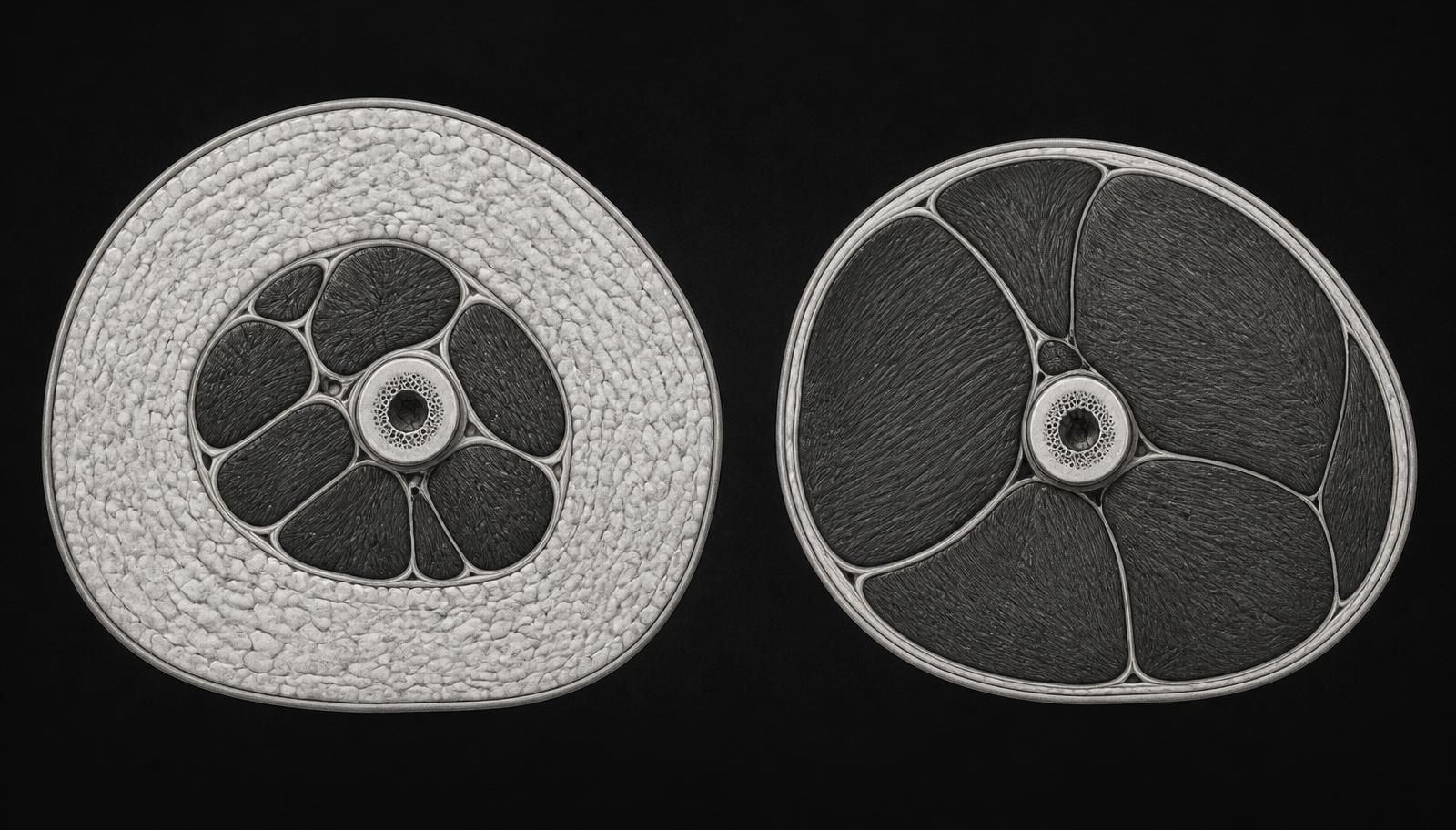
Pale ring = adipose tissue
Dark mass = lean muscle
Repair One · Skeletal muscle
Muscle is a metabolic organ — not just movement.
Skeletal muscle is the body's largest site of glucose disposal, a reservoir for amino acids, and a driver of resting metabolic rate. Losing it accelerates almost every marker of aging.
Resistance training reverses muscle loss in midlife.
Progressive resistance training increases muscle mass, strength, and function in older adults — including in very old and previously untrained populations. It is the single most effective intervention against sarcopenia.
Low muscle mass tracks with higher mortality.
In large cohorts, low muscle mass and low strength are independently associated with higher all-cause mortality — often more predictive than body weight or BMI alone.
Repair Two · Cardiovascular muscle
VO₂ max is the single strongest predictor of how long you live.
VO₂ max is the maximum volume of oxygen your heart, lungs, and capillary network can deliver to working tissue — the cardiovascular equivalent of a one-rep max. The way we raise it is simple: one or two short interval sessions per week (four minutes hard, three minutes easy, repeated four times — the "Norwegian 4×4"), plus easy zone-2 aerobic work on the other days.
Sedentary · low VO₂ max
Endurance-trained · high VO₂ max
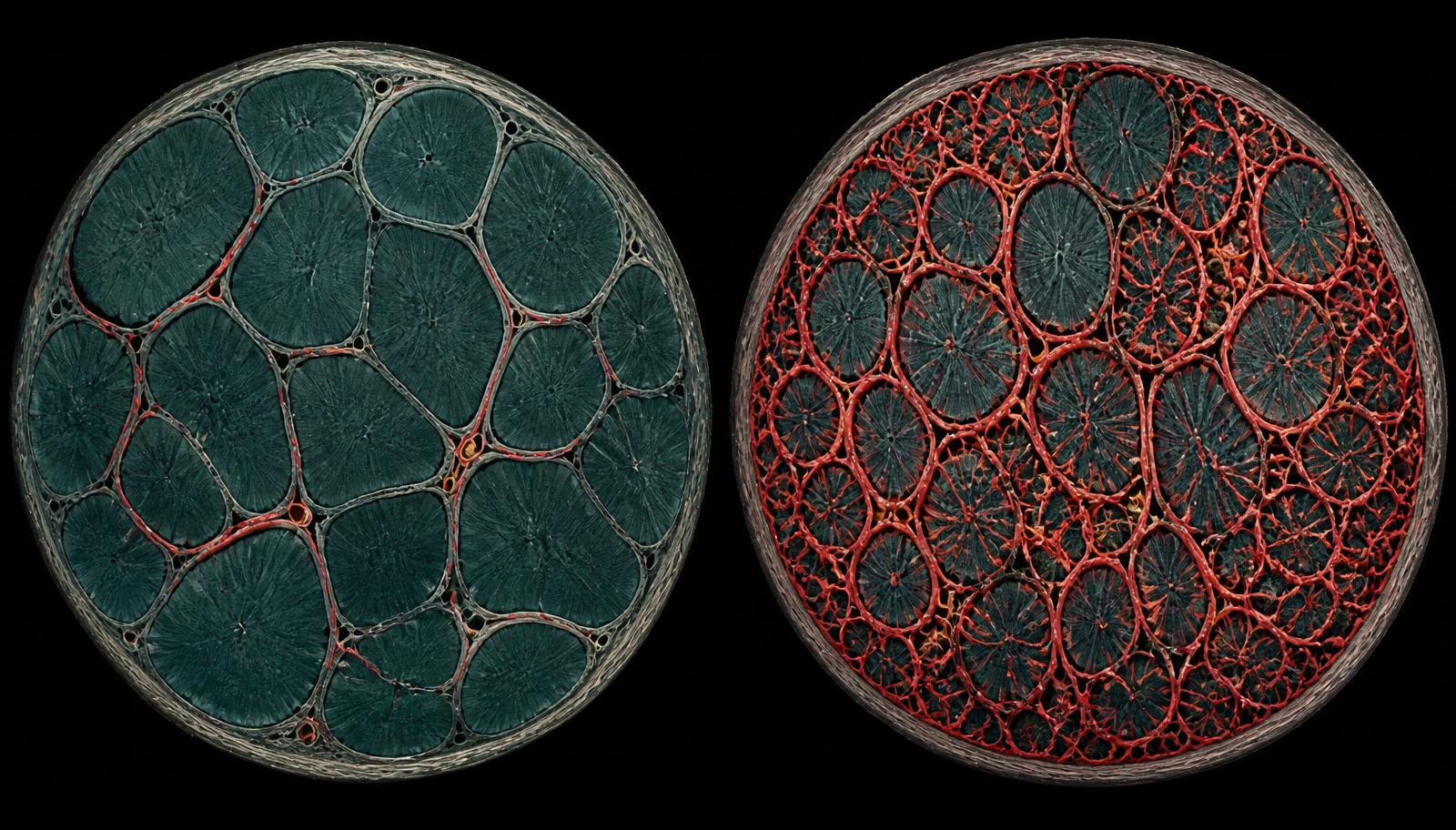
Sparse red web = few capillaries
Dense red web = oxygen delivery
Low fitness carries a mortality risk comparable to smoking or diabetes.
In 122,007 adults on treadmill testing, low cardiorespiratory fitness carried a mortality risk on par with smoking, diabetes, and coronary artery disease. Elite VO₂ max was associated with a five-fold lower risk of death vs. low fitness.
Every step up in fitness drops your risk of dying.
Meta-analysis of 33 studies (over 100,000 participants): every 1-MET improvement in cardiorespiratory fitness lowered all-cause mortality by 13% and cardiovascular events by 15%. Fitness is dose-responsive.
Twelve weeks of 4×4 intervals raises VO₂ max by ~15%.
In previously sedentary adults, twelve weeks of the Norwegian 4×4 interval protocol raised VO₂ max by roughly 15% and dropped blood pressure meaningfully. It's the protocol behind the interval prescription above.
Recommended · Read
Dr. Gabrielle Lyon — Forever Strong.
Jorge's go-to reference on muscle-centric medicine. Lyon reframes the conversation: we don't have an obesity problem, we have a muscle problem.
Find it on Amazon →
Bonus · Watch
Sarcopenia — with Robb Wolf.
Jorge and Robb Wolf on why age-related muscle loss is the quiet driver of decline — and how to reverse it. (Aired as Ozempic: Miracle or Muscle Killer?)
Watch it on Substack →
03 · The Mineral–Hunger Connection
Much of what you call hunger is a mineral signal.
Modern diets and fasting both deplete sodium, potassium, and magnesium. When those minerals run low, the body doesn't ask for them directly — it ramps up the drive to eat. Replace what's missing, and a large share of that "hunger" quiets at its source.
Low sodium drives salt- and food-seeking.
When sodium is depleted, the brain's drive toward salt and palatable food rises sharply — a well-mapped physiology, not a theory.
Magnesium steadies blood sugar — and steadier blood sugar means fewer cravings.
In randomized trials, oral magnesium improved insulin sensitivity and fasting glucose. About half of U.S. adults fall short of the magnesium target.
Electrolytes make fasting livable.
Replacing sodium, potassium, and magnesium relieves the fatigue, headache, and hunger that derail a fast — which is why most members sip minerals across their fasting window rather than reaching for food.
04 · The Turning Point — GLP-1 vs Minerals
GLP-1 works — until the body adapts.
Every powerful weight-loss tool runs into the same wall: the body fights back. GLP-1 medications produce strong appetite suppression at first, but the effect plateaus around 60–72 weeks — and when the medication stops, most of the lost weight returns, roughly two-thirds within a year. Even bariatric surgery, the most powerful option, sees meaningful regain over time. This is metabolic adaptation, and it applies to nearly every approach.
Restoring minerals is different. Sodium, potassium, and magnesium are nutrients the body needs daily — there is no known tolerance or "adaptation" to them. As long as the deficiency is corrected, the effect holds. That is the quiet advantage of the protocol: durability and simplicity, not a larger drop on the scale.
Illustrative comparison of approaches — not a claim of equivalent results.
| A time-restricted-eating lifestyle (with Zero Hunger Water) | GLP-1 medication | Bariatric surgery | |
|---|---|---|---|
| Monthly cost | Cost of a daily drink | Typically $$$–$$$$ per month | Large one-time surgical cost |
| Prescription required | No | Yes | Yes — plus surgical eligibility |
| Injections | None | Weekly self-injection | N/A (surgery) |
| Common side effects | None expected | Nausea, GI issues, fatigue commonly reported | Surgical risk; lifelong nutrient monitoring |
| Muscle-mass impact | Supports muscle when paired with resistance training + protein | Muscle loss commonly reported with rapid weight loss | Muscle loss common with rapid weight loss |
| Medical supervision | Optional — talk to your doctor if you have kidney, heart, or blood-pressure conditions | Required — prescribed and monitored by a clinician | Required — surgical team + lifelong follow-up |
| Sustainability | Designed to be a daily habit for life | Effect typically fades if the medication is stopped | Durable, though some regain is common over years |
Illustrative comparison of approaches. Not a claim of equivalent results. The comparison contrasts three routes a person could choose; it does not plot pounds, inches, BMI, or percent body weight. Gastric bypass remains the most effective medical option for weight loss. Individual experience varies. These statements have not been evaluated by the Food and Drug Administration. Zero Hunger Water is not intended to diagnose, treat, cure, or prevent any disease.
Important
Zero Hunger Water does not contain GLP-1 and is not a GLP-1 drug or a substitute for one. Always talk to your doctor before starting, changing, or stopping any medication.
05 · The Studies — Reference Materials
References
- 01Morris MJ, Na ES, Johnson AK. Salt craving: the psychobiology of pathogenic sodium intake. Physiology & Behavior. 2008. PMID 18514747. →
- 02Meta-analysis of randomized controlled trials: oral magnesium supplementation, insulin sensitivity and fasting glucose. 2016. PMID 27530471. →
- 03He M, et al. Time-restricted eating with or without low-carbohydrate diet reduces visceral fat and improves metabolic syndrome: a randomized trial. Cell Reports Medicine. 2022. PMID 36220069. →
- 04Cerhan JR, et al. Waist circumference and all-cause mortality. Mayo Clinic Proceedings. 2014. PMID 24582192. →
- 05Katzmarzyk PT, et al. Waist circumference and mortality risk. Archives of Internal Medicine. 2009. →
- 06Stanhope KL, et al. Fructose-sweetened beverages, visceral adiposity and insulin sensitivity. Journal of Clinical Investigation. 2009. PMID 19381015. →
- 07Wilding JPH, et al. (STEP-1) Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine. 2021. →
- 08Jastreboff AM, et al. (SURMOUNT-1) Tirzepatide once weekly for obesity. New England Journal of Medicine. 2022. →
- 09Wilding JPH, et al. (STEP-1 extension) Weight regain after withdrawal of semaglutide. Diabetes, Obesity & Metabolism. 2022. PMID 35441470. →
- 10(SURMOUNT-4) Continued versus withdrawn tirzepatide and weight maintenance. JAMA. 2024. →
- 11Hall KD. Metabolic adaptations to weight loss across diet, drug, and surgery. Obesity. 2024. →
- 12Wolfe RR. The underappreciated role of muscle in health and disease. American Journal of Clinical Nutrition. 2006. PMID 16960159. →
- 13Liu CJ, Latham NK. Progressive resistance strength training for improving physical function in older adults. Cochrane Database of Systematic Reviews. 2009. PMID 19588334. →
- 14Srikanthan P, Karlamangla AS. Muscle mass index as a predictor of longevity in older adults. American Journal of Medicine. 2014. PMID 24561114. →
- 15Lyon G. Forever Strong: A New, Science-Based Strategy for Aging Well. Atria Books, 2023. Recommended reading. →
Most hunger isn't hunger. It's a mineral deficiency.
*Illustrative — not a claim of specific results. All graphics on this page (visceral-fat animation, muscle cross-section, and adaptation chart) are educational illustrations, not depictions of a specific individual's outcome.
Important: Zero Hunger Water does not contain GLP-1 and is not a GLP-1 drug or a substitute for one. These statements have not been evaluated by the Food and Drug Administration. This protocol is not intended to diagnose, treat, cure, or prevent any disease, and is not a substitute for medical care or prescribed medication. The comparison above is illustrative and is not based on a head-to-head study of these three approaches. Never start, stop, or change a medication without your doctor. If you have kidney disease, high blood pressure, heart failure, or take medications that affect potassium (ACE inhibitors, ARBs, or potassium-sparing diuretics), talk with your doctor before increasing your mineral intake.